Ectopic Pregnancy
Life-threatening cause of first-trimester pain and bleeding. A positive pregnancy test + pain/bleeding = ectopic until proven intra-uterine.
Early pregnancy + pain/bleeding
Always do β-hCG
Pregnancy of unknown location
Unstable → theatre
ED Priorities
Overview
Key concept: Any reproductive-age woman with positive pregnancy test and abdominal pain and/or vaginal
bleeding has an ectopic pregnancy until proven otherwise. Your first job is to recognise rupture and prevent
maternal collapse.
- Peak incidence in first trimester, most commonly 6–8 weeks from last menstrual period.
- Most ectopics are tubal (ampullary); rupture causes intra-abdominal haemorrhage and shock.
- Early diagnosis and gynae involvement reduce morbidity and mortality.
ED Algorithm
Flow- Check vitals, ABC. If shocked (tachycardia, hypotension, pallor, syncope) → resuscitate and call gynae immediately.
- Confirm pregnancy: urine or serum β-hCG in all reproductive-age women with pain/bleeding.
- Take focused history (LMP, pain onset and site, bleeding amount, risk factors, contraception, previous ectopic or PID).
- Examine:
- Abdomen – tenderness, guarding, rebound, distension.
- Pelvic exam if appropriate – cervical motion tenderness, adnexal mass, uterine size, amount of bleeding.
- Send baseline bloods: FBC, U&E, group & save ± cross-match, ± coagulation; consider ABG if unwell.
- Perform ultrasound (ideally transvaginal) as soon as feasible:
- Intrauterine pregnancy (IUP) seen → ectopic unlikely but heterotopic still possible in IVF/high-risk.
- No IUP + positive β-hCG → pregnancy of unknown location (PUL) → ectopic until proven otherwise.
- Unstable or high suspicion of rupture at any point → urgent gynae consult for surgical management.
- Stable PUL → arrange serial β-hCG and repeat scan in collaboration with gynae/early pregnancy clinic.
Risk Factors
Who’s High Risk?Ectopics can occur in patients with no risk factors, but risk is higher in:
- Previous ectopic pregnancy.
- Previous tubal surgery or tubal ligation / reconstruction.
- Pelvic inflammatory disease, chlamydia or other STIs causing tubal damage.
- Infertility and assisted reproductive techniques (e.g. IVF).
- Current or recent IUD use (if pregnancy occurs despite IUD, ectopic risk is higher).
- Smoking.
- Advanced maternal age (> 35 years).
- History of spontaneous or induced abortion (often reflecting underlying tubal pathology).
Tip for juniors: A “low risk” history does not rule out ectopic. Never skip the pregnancy test.
Clinical Presentation
Symptoms & SignsPresentation is often subtle and variable. Maintain a high index of suspicion.
- Classic triad: missed/late period + lower abdominal pain + vaginal bleeding (but all three may not be present).
- Unilateral pelvic pain, often crampy or sharp.
- Light to moderate vaginal bleeding or brown discharge.
- Shoulder tip pain or diaphragmatic irritation if significant intra-abdominal blood.
- Dizziness, pre-syncope, syncope – especially if rupture and blood loss.
- On exam: adnexal tenderness or mass, cervical motion tenderness, uterine size smaller than expected.
Red flags for rupture: sudden severe abdominal pain, collapse, tachycardia, hypotension, abdominal distension,
shoulder pain → treat as ruptured ectopic and call gynae/theatre urgently.
Diagnostic Tools
Workup- β-hCG (serum):
- Confirms pregnancy and helps interpret ultrasound.
- In a viable IUP, β-hCG should typically rise appropriately over 48 hours; plateauing or slow rise raises concern for ectopic or failing pregnancy.
- Transvaginal ultrasound (TVUS):
- Preferred imaging modality – detects IUP, adnexal mass, yolk sac, fetal pole, free fluid.
- Absence of IUP when β-hCG is above the local “discriminatory zone” (often around 1500–2000 IU/L) is highly suspicious for ectopic or PUL.
- Abdominal ultrasound: less sensitive but useful where TVUS unavailable – look for free fluid, obvious adnexal mass.
- Serial β-hCG measurements: especially important in stable PUL – rising, falling, or plateauing patterns guide further management.
- Laparoscopy: definitive diagnosis and treatment when imaging is inconclusive and suspicion remains high, or when patient is unstable.
Management in the ED
Emergency
Principle: Resuscitate and stabilise first, then decide between surgical and medical management with gynae.
Unstable = surgery. Stable = individualised.
1. Haemodynamically Unstable / Ruptured Ectopic
- Immediate ABC assessment; high-flow oxygen.
- Two large-bore IV lines; send bloods including cross-match.
- Fluid resuscitation with crystalloid while arranging blood products.
- Activate massive transfusion if major haemorrhage suspected.
- Urgent gynae consult – emergency laparotomy/laparoscopy for haemostasis and removal of ectopic.
- Keep NBM; prepare for theatre; continuous monitoring.
2. Haemodynamically Stable – Surgical vs Medical
- Surgical options: laparoscopy (salpingostomy or salpingectomy) or laparotomy depending on local resources and patient factors.
- Medical management (methotrexate): usually considered when:
- Patient is stable and reliable for follow-up.
- No evidence of rupture or significant haemoperitoneum.
- β-hCG relatively low (local cut-off varies; often < 5000 IU/L).
- No fetal cardiac activity and small ectopic size on TVUS.
- No contraindications to methotrexate (e.g. liver disease, breastfeeding, immunodeficiency, renal failure).
- Methotrexate protocols and follow-up schedules are usually managed by gynae/early pregnancy services.
3. Pregnancy of Unknown Location (PUL)
- Positive pregnancy test + no IUP or ectopic seen on scan.
- Stable patients can often be managed as outpatient with:
- Serial β-hCG (typically 48-hour intervals).
- Repeat TVUS as arranged by gynae/early pregnancy clinic.
- Provide clear written instructions and emergency return advice.
Complications & Follow-Up
Aftercare- Immediate complications: haemorrhagic shock, need for transfusion, anaesthetic risk.
- Long-term concerns: reduced fertility (especially after salpingectomy), risk of recurrent ectopic, psychological impact.
- Patients treated with methotrexate:
- Require repeated β-hCG monitoring until undetectable.
- Must avoid pregnancy and folate supplements until cleared by gynae.
- All patients should receive clear follow-up plans with gynae/early pregnancy services.
Patient Counselling & Education
Communication- Explain in simple terms what an ectopic pregnancy is and why it cannot continue safely.
- Emphasise the risk of rupture and need for urgent treatment – this is about protecting the patient’s life.
- Discuss:
- Which treatment was chosen (surgical vs medical) and why.
- Expected symptoms and side-effects.
- When to seek urgent care – worsening pain, dizziness, collapse, heavy bleeding.
- Acknowledge emotional impact and offer support / referral for counselling if available.
- Discuss future pregnancy planning and the importance of early assessment in subsequent pregnancies.
Always test for pregnancy
Positive test + pain/bleeding → ectopic until proven otherwise
Unstable → immediate gynae/theatre
Stable PUL → serial β-hCG + TVUS
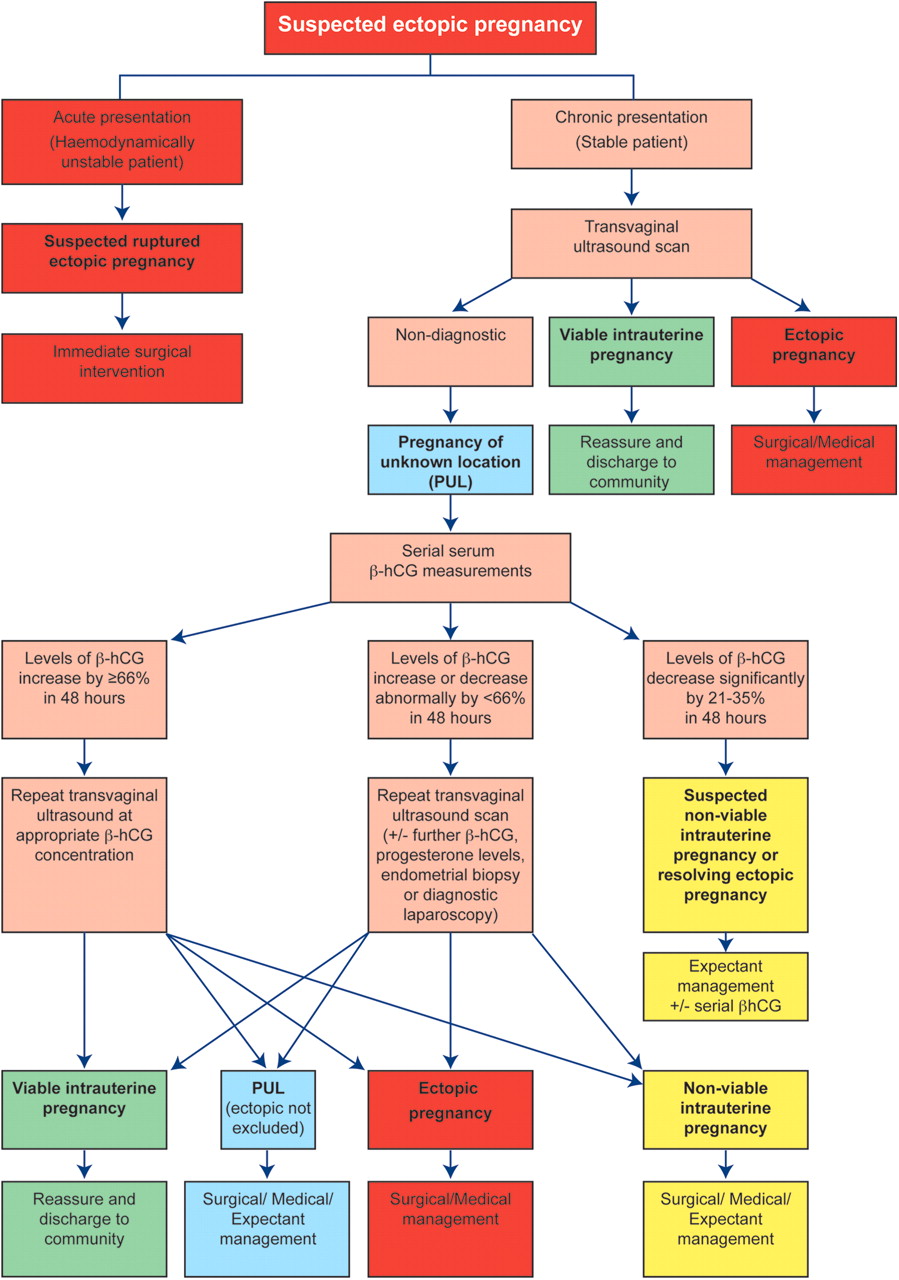
Ectopic Pregnancy Algorithm
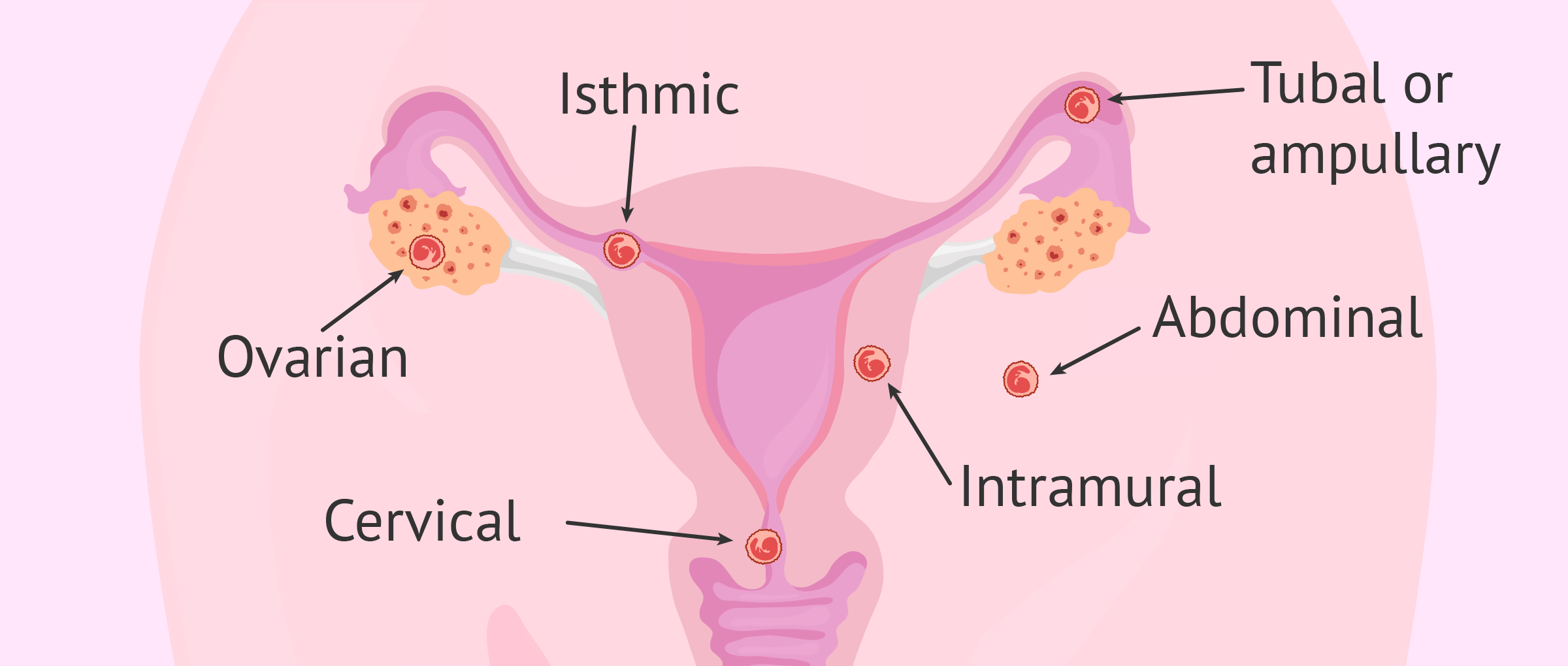
Types of Ectopic Pregnancies