1. When to Suspect Spinal Injury
If in doubt, immobilise and image – especially with high-energy mechanisms.
- High-risk mechanism:
- High-speed RTC, rollover, ejection
- Pedestrian/cyclist struck by vehicle
- Fall > 1 m / > 5 stairs
- Axial load to head (e.g. diving injury)
- Neurological symptoms:
- Paraesthesia, weakness, paralysis
- Loss of anal tone, urinary retention or incontinence
- Midline spinal tenderness on palpation
- Distracting injuries (e.g. long bone fracture, major chest/abdominal trauma)
- Intoxication or reduced level of consciousness (GCS < 15)
- Known vertebral disease (e.g. ankylosing spondylitis, severe osteoporosis)
2. Immediate Actions in ED
- Maintain spinal motion restriction:
- Manual in-line stabilisation initially
- Rigid collar, blocks and tape (or in-line hands) as per local protocol
- Avoid log-rolling without adequate team and control
- Follow ATLS A–B–C–D–E – do not delay life-saving interventions for imaging.
- Document time spinal precautions applied and by whom.
3. Clearing the Cervical Spine (Adult)
Use a validated rule (Canadian C-Spine or NEXUS) and local protocols.
Canadian C-Spine Rule (simplified)
- High-risk factors → Image C-spine
- Age ≥ 65 years
- Dangerous mechanism (high-speed RTC, fall > 1 m/5 stairs, axial load, etc.)
- Paraesthesia in extremities
- If NO high-risk factors, check low-risk factors:
- Simple rear-end MVC
- Patient sitting in ED; ambulatory at any time
- Delayed onset neck pain
- No midline cervical tenderness
- If low-risk factors present → patient can actively rotate neck 45° left and right?
- Yes: C-spine can be clinically cleared
- No: Image C-spine (CT preferred in trauma)
NEXUS Low-Risk Criteria
C-spine can be cleared clinically if ALL of the following are true:
- No posterior midline cervical tenderness
- No focal neurological deficit
- Normal level of alertness (GCS 15)
- No intoxication
- No painful distracting injury
If patient is intubated, confused, intoxicated or poly-trauma → assume spinal injury until CT and specialist review.
4. Focused Examination
- Inspect: deformity, bruising, step-offs, wounds along the spine.
- Palpate: midline tenderness, gaps/steps; paraspinal muscle spasm.
- Motor: power in all major muscle groups (upper and lower limbs).
- Sensation: light touch and pain in all dermatomes; perianal sensation.
- Reflexes: deep tendon reflexes, Babinski.
- ASIA classification if time/setting allows (particularly for SCI).
5. Red Flag Features – Spinal Cord / Cauda Equina
These are emergencies – discuss with neurosurgery/orthopaedics urgently.
- Bilateral leg weakness or rapidly progressive weakness RED FLAG
- Loss of anal tone or saddle anaesthesia RED FLAG
- Urinary retention, overflow incontinence, or faecal incontinence RED FLAG
- Severe midline back pain with neurological deficit RED FLAG
- High thoracic/cervical injuries with hypotension + bradycardia (neurogenic shock)
6. Imaging – When and What
- CT spine:
- Preferred modality in moderate / severe trauma
- Any failed clinical clearance (Canadian/NEXUS)
- GCS < 15, intoxicated, or distracting injuries
- Plain X-rays:
- Low-resource settings / low-risk patients only
- Must visualise all relevant vertebrae and junctions
- MRI:
- Neurological deficit with normal CT
- Suspected cord injury, epidural haematoma, disc prolapse
7. Ongoing Management in ED
- Maintain spinal precautions until cleared by appropriate imaging and senior review.
- Aggressive treatment of hypotension and hypoxia – spinal cord is very vulnerable.
- Adequate analgesia and anti-spasm measures.
- Pressure care: regular checks to avoid pressure sores in immobilised patients.
- Early discussion with:
- Orthopaedics / neurosurgery
- ICU for high cervical injuries or respiratory compromise
- Clear documentation:
- Mechanism, exam findings, neurological status
- Time of collar application and clearance
- Imaging performed and specialist plans
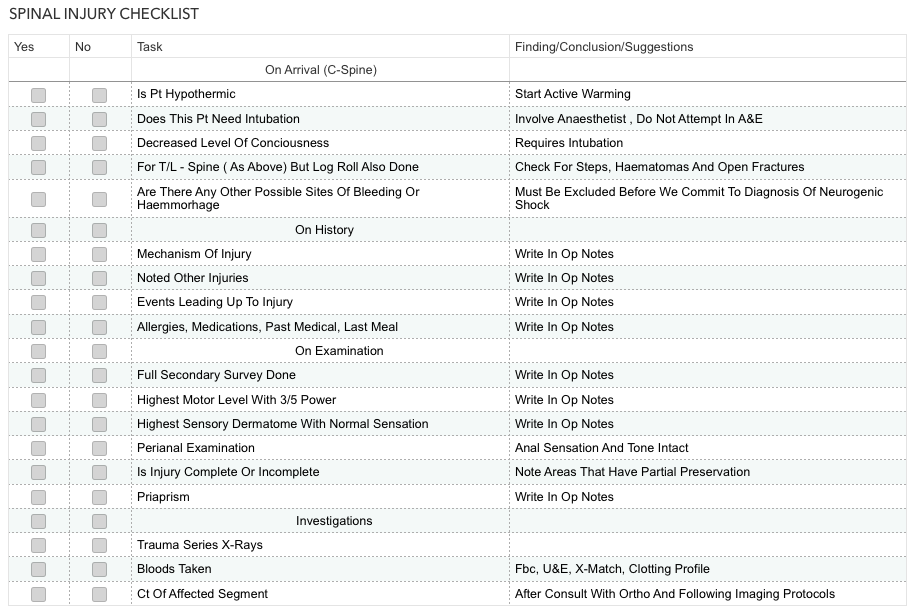
Original Spinal Injury Checklist poster
(Tap to enlarge)