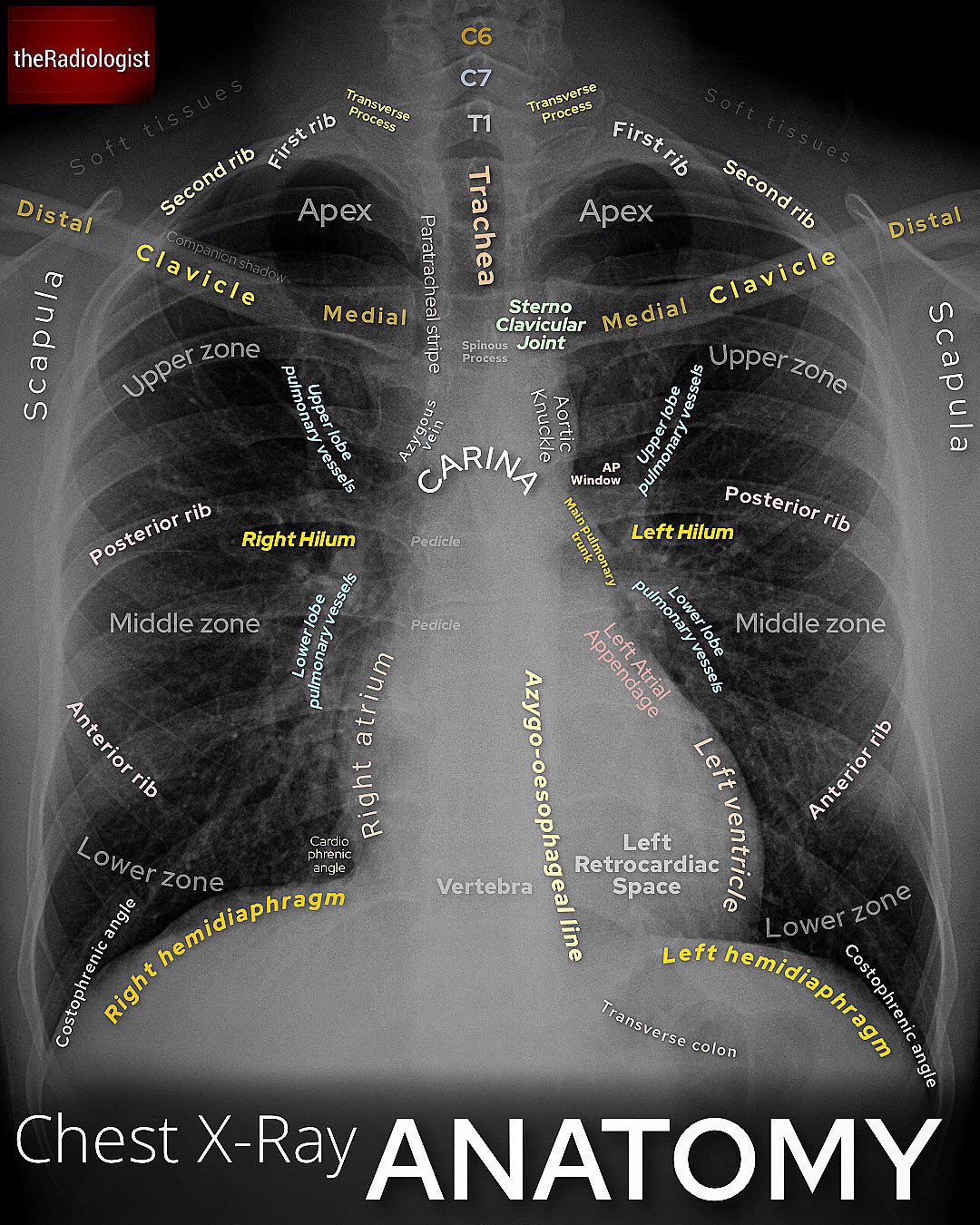
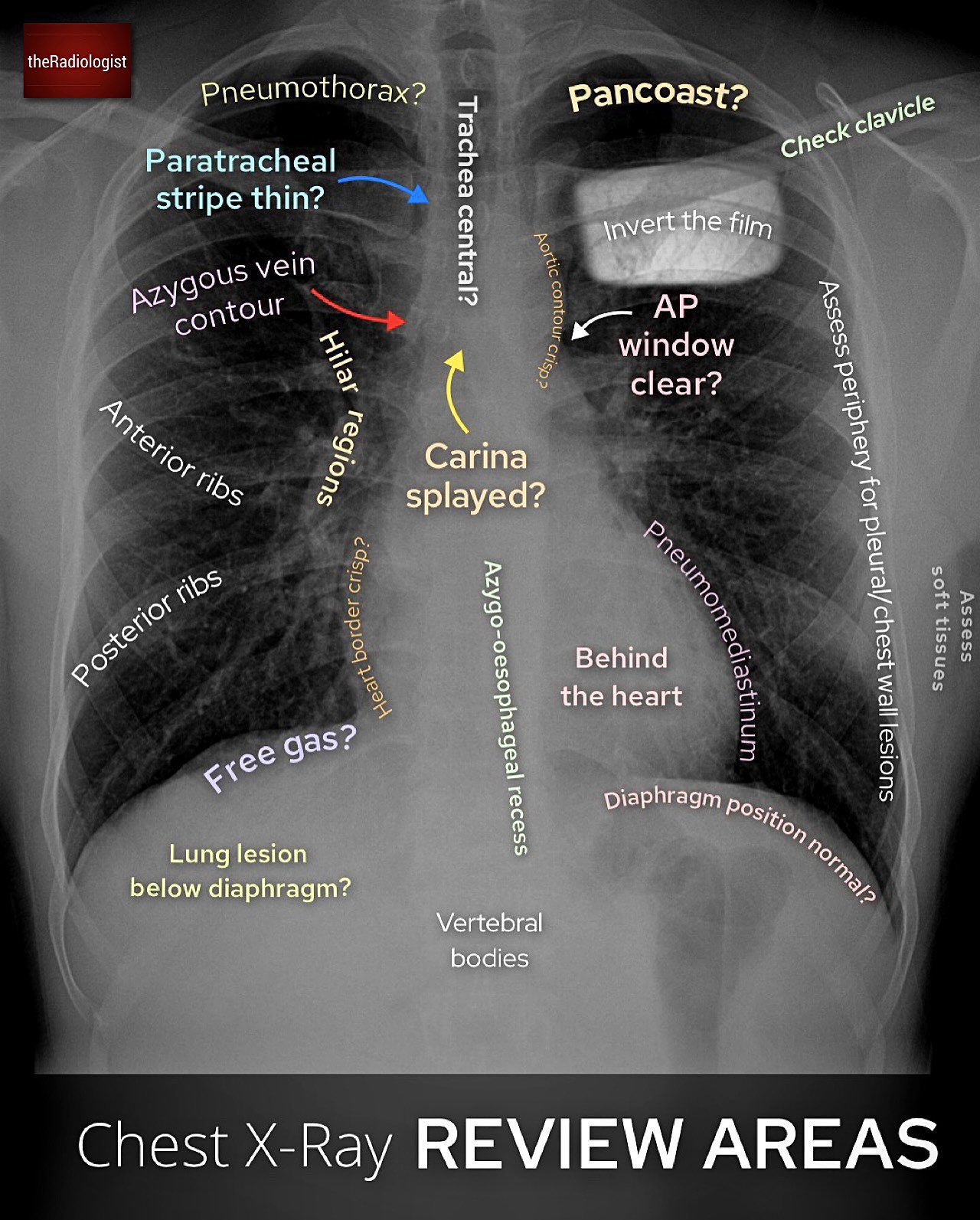
When analysing a chest X-ray, a systematic approach helps ensure that no important findings are missed.
One simple way is to move from image quality → bones/soft tissues → lungs → mediastinum/heart →
pleura/diaphragm.
Check patient details and image quality
Confirm name, date of birth, and study date.
Check penetration, rotation, and inspiration (ideally 9–10 posterior ribs visible).
Assess bones and soft tissues
Look for fractures, dislocations, lytic/sclerotic lesions.
Scan soft tissues for masses, swelling, subcutaneous emphysema, or foreign bodies.
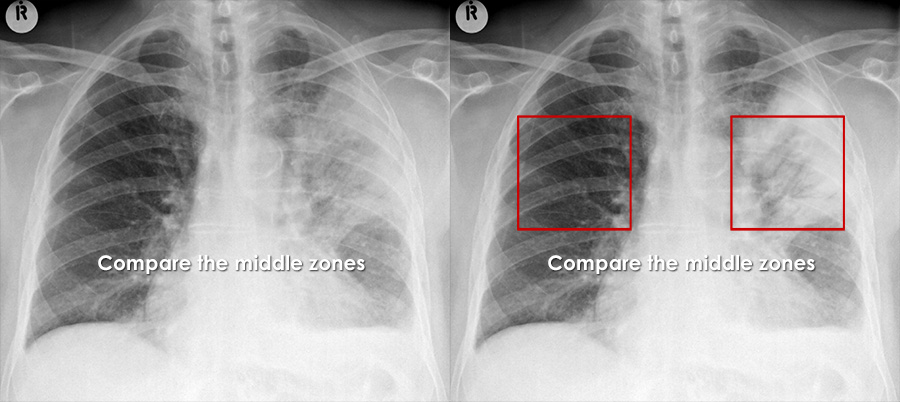
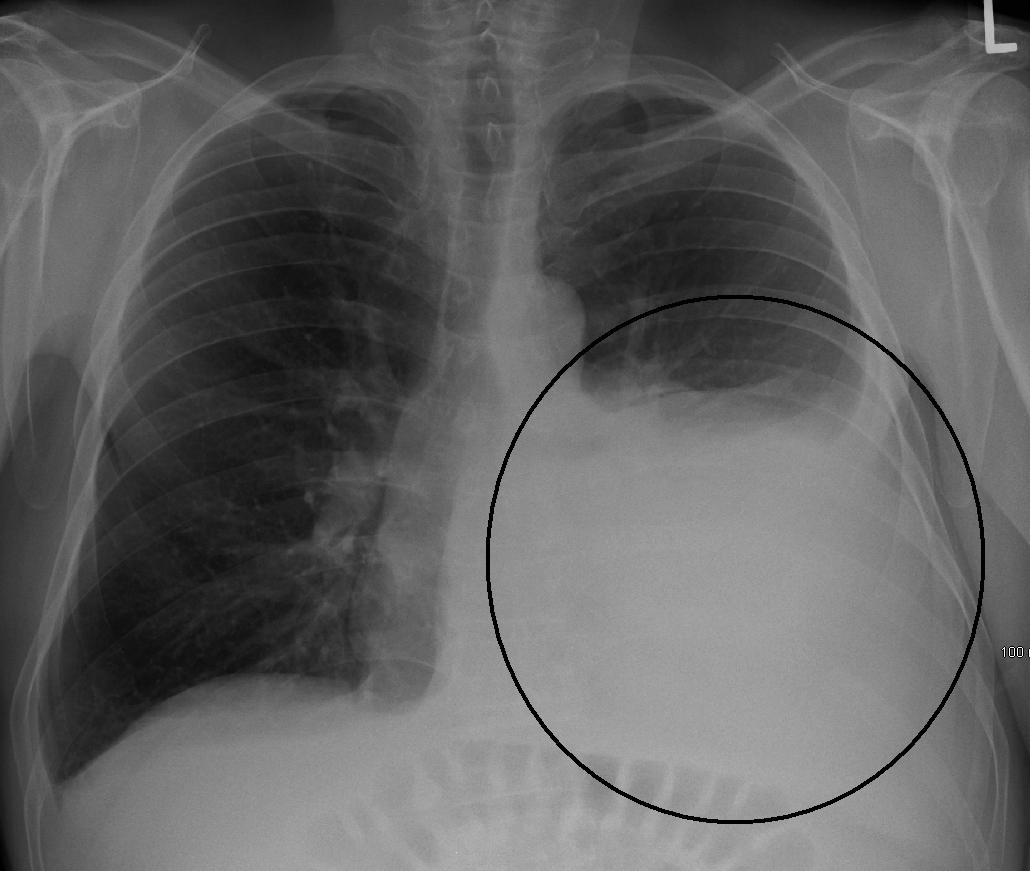
Examine the lung fields
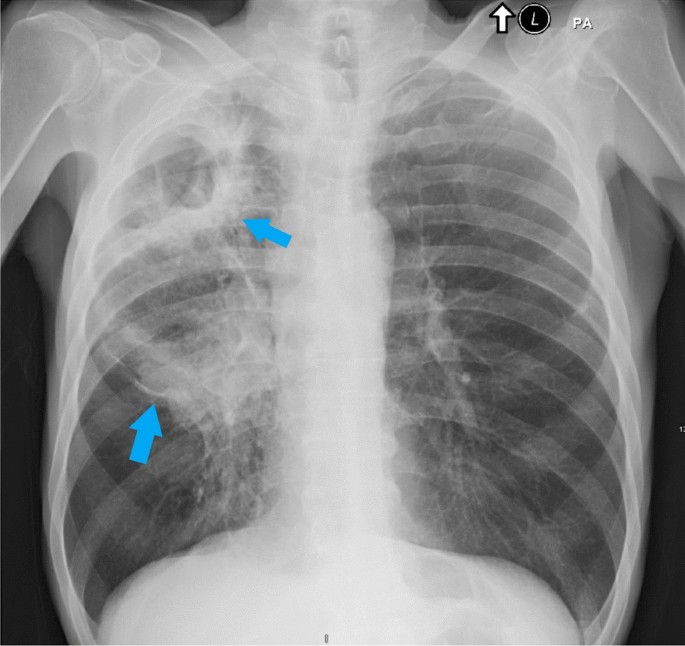
Consolidation, masses, nodules, cavities.
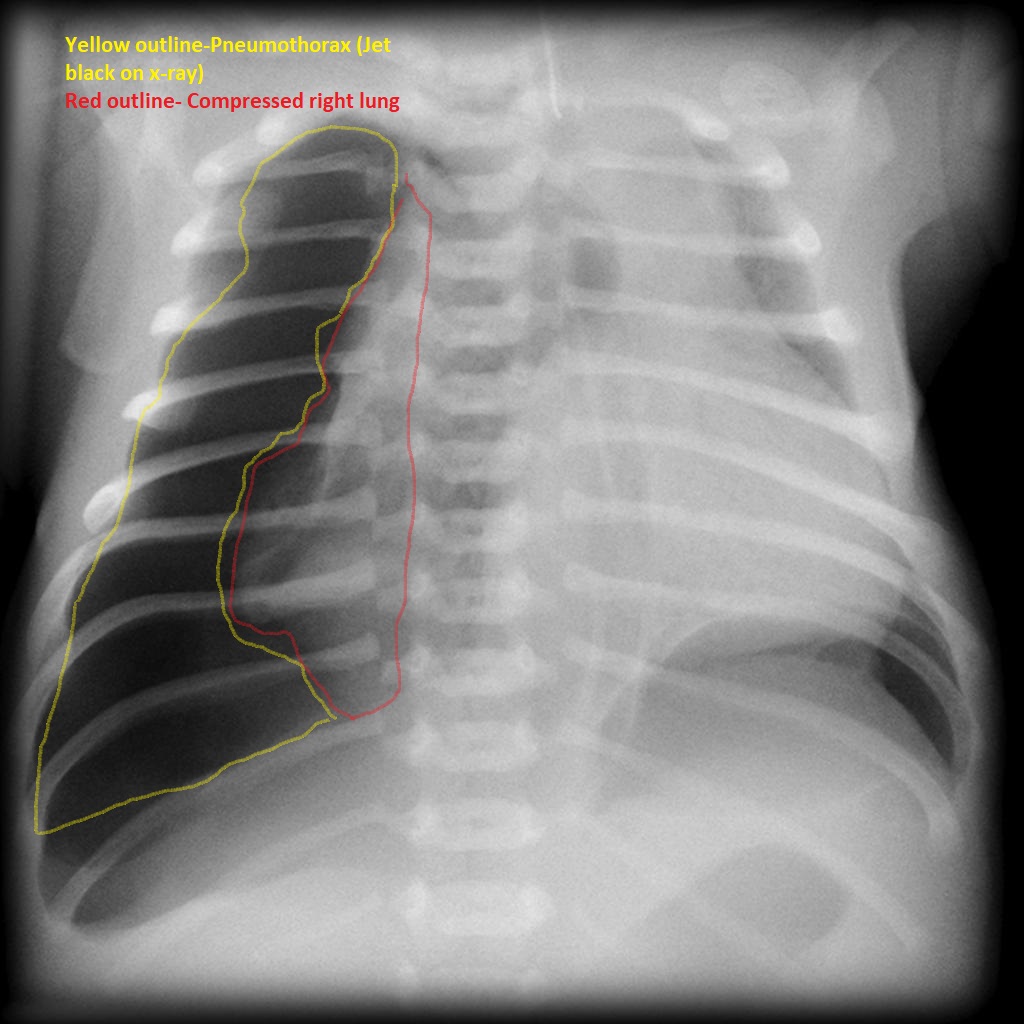
Signs of atelectasis (volume loss, shift) or pneumothorax.
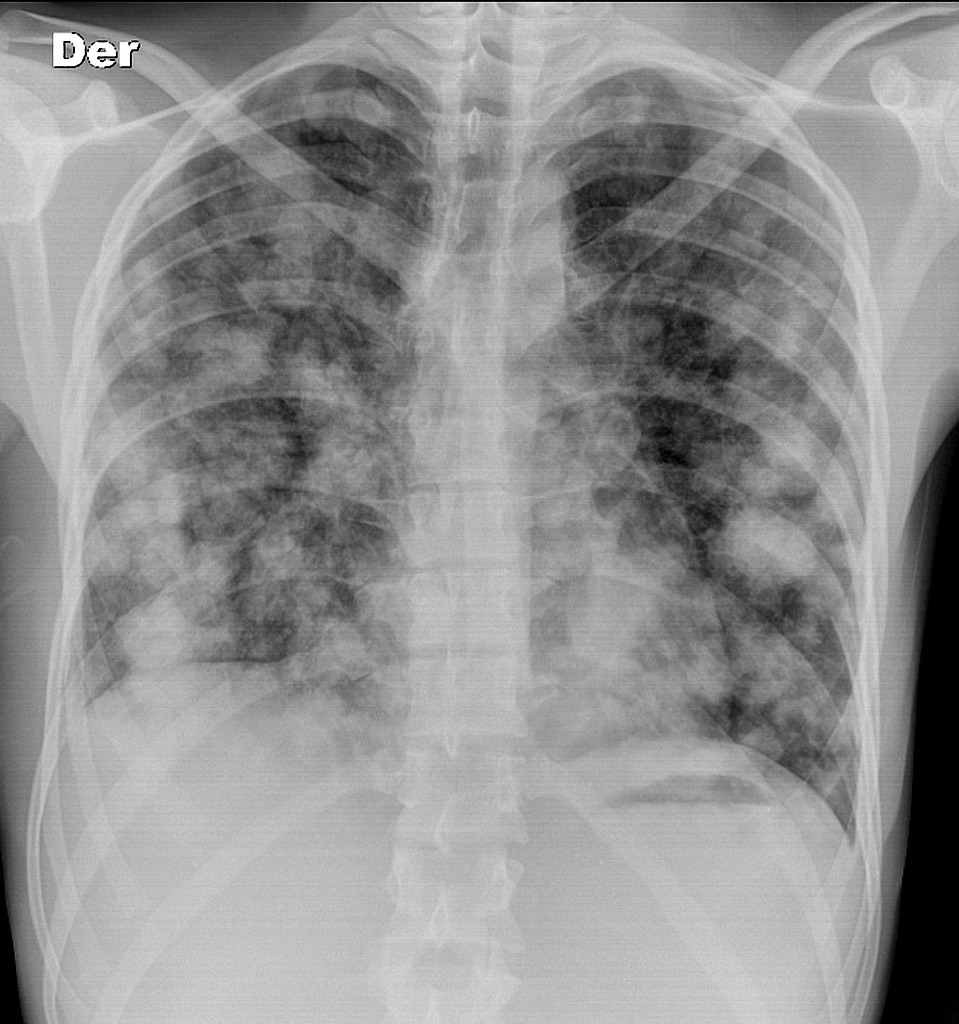
Diffuse tiny nodules throughout both lungs (miliary pattern).
May have associated involvement of liver, spleen, brain, etc.
Diagnostic Clues
Positive TST or IGRA.
Sputum AFB smear/culture or molecular tests.
CXR pattern consistent with TB, interpreted with clinical context.
Treatment requires combination anti-TB therapy over several months according to national guidelines.
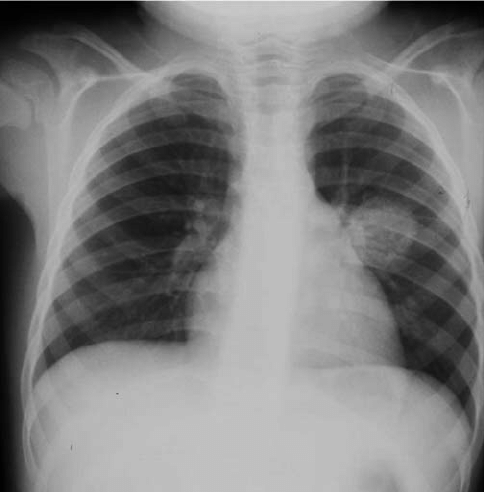
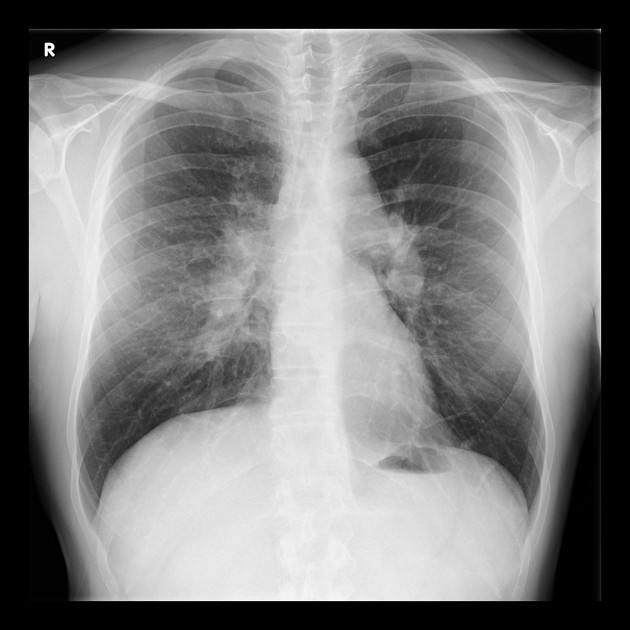
Latent TB – often normal CXRActive pulmonary TBGhon complex on CXRMiliary TB
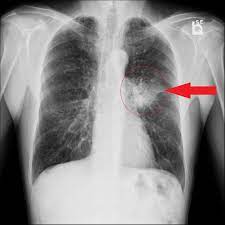
Lung Cancer
Lung Cancer Type
Radiological Features
Non–small cell lung cancer (NSCLC)
Solitary nodule or mass, irregular/spiculated margins, possible cavitation.
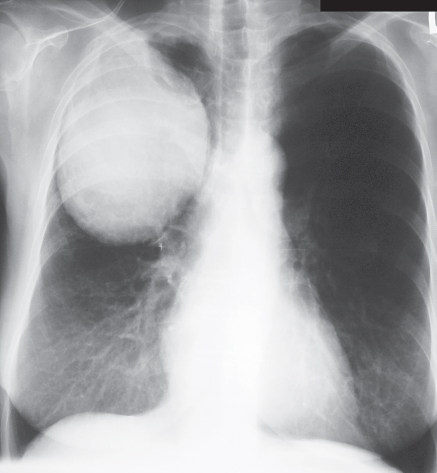
Small cell lung cancer (SCLC)
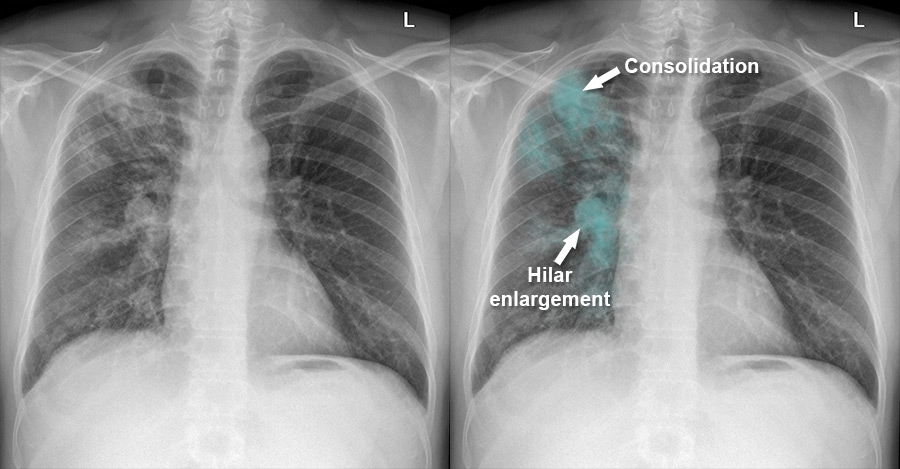
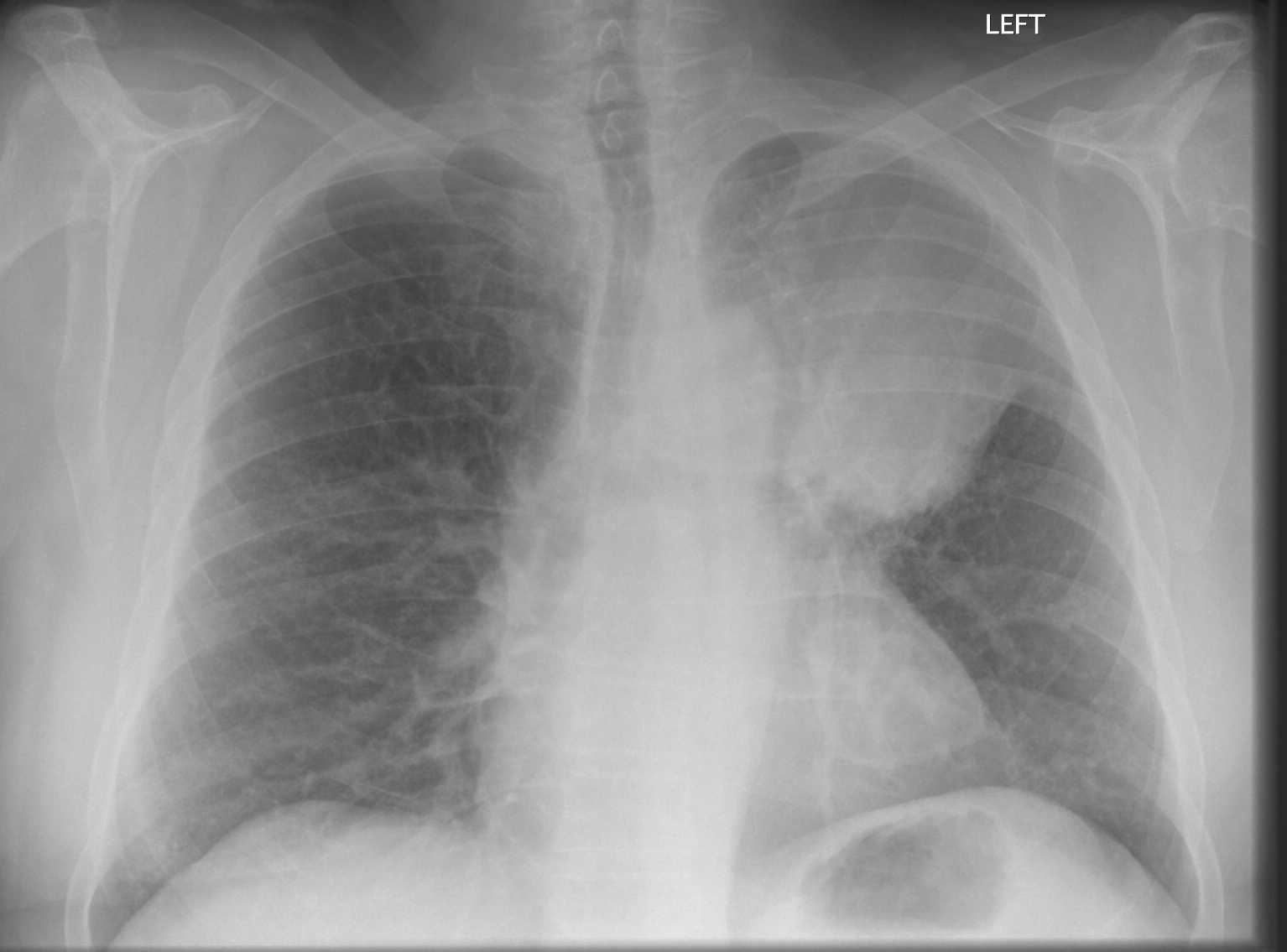
Central or hilar mass, rapid growth, prominent lymphadenopathy.
Adenocarcinoma
Peripheral nodule, sometimes ground-glass opacity or lepidic growth pattern.
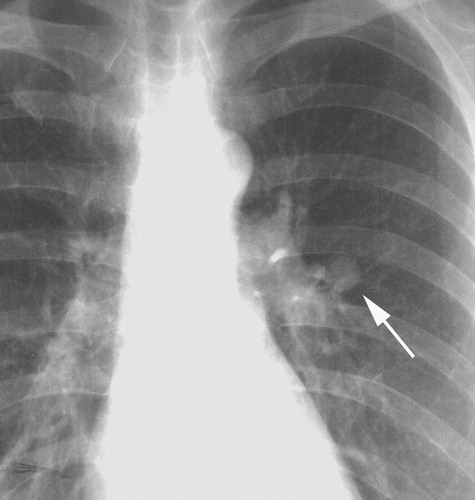
Squamous cell carcinoma
Central mass or nodule, frequent cavitation, hilar lymphadenopathy.
Large cell carcinoma
Peripheral or central mass, rapid growth, may cavitate.
Bronchial carcinoid tumour
Well-defined, round/oval nodule; central or peripheral; usually slow-growing.
Metastases to the lung
Multiple nodules of varying size, well-defined margins, random distribution; may cavitate depending on primary.
Non–small cell lung cancer (NSCLC)Small cell lung cancer (SCLC)Adenocarcinoma of the lungSquamous cell carcinoma of the lungLarge cell carcinoma of the lungBronchial carcinoid tumourMetastatic deposits in the lung
Final Note
This page provides a rapid overview of common CXR patterns for ED practice. Always integrate radiographic
findings with clinical assessment, lab results, and further imaging where indicated, and discuss
uncertainties with radiology or a senior colleague.