Basic CT Brain and C-Spine Analysis for Junior Doctors
Introduction
CT scans are commonly used to evaluate patients with suspected brain or cervical spine injury. As a junior doctor, having a structured approach to CT analysis helps with early recognition of life-threatening pathology and improves communication with radiology and the trauma team.
CT Brain Analysis – Key Features
When reviewing a CT brain, systematically look for:
- Midline shift: Displacement of midline structures (falx cerebri, septum pellucidum) suggests mass effect from haemorrhage, tumour or major oedema.
- Haemorrhage: Hyperdense areas. Classify as epidural, subdural, intraparenchymal, or subarachnoid based on location and shape.
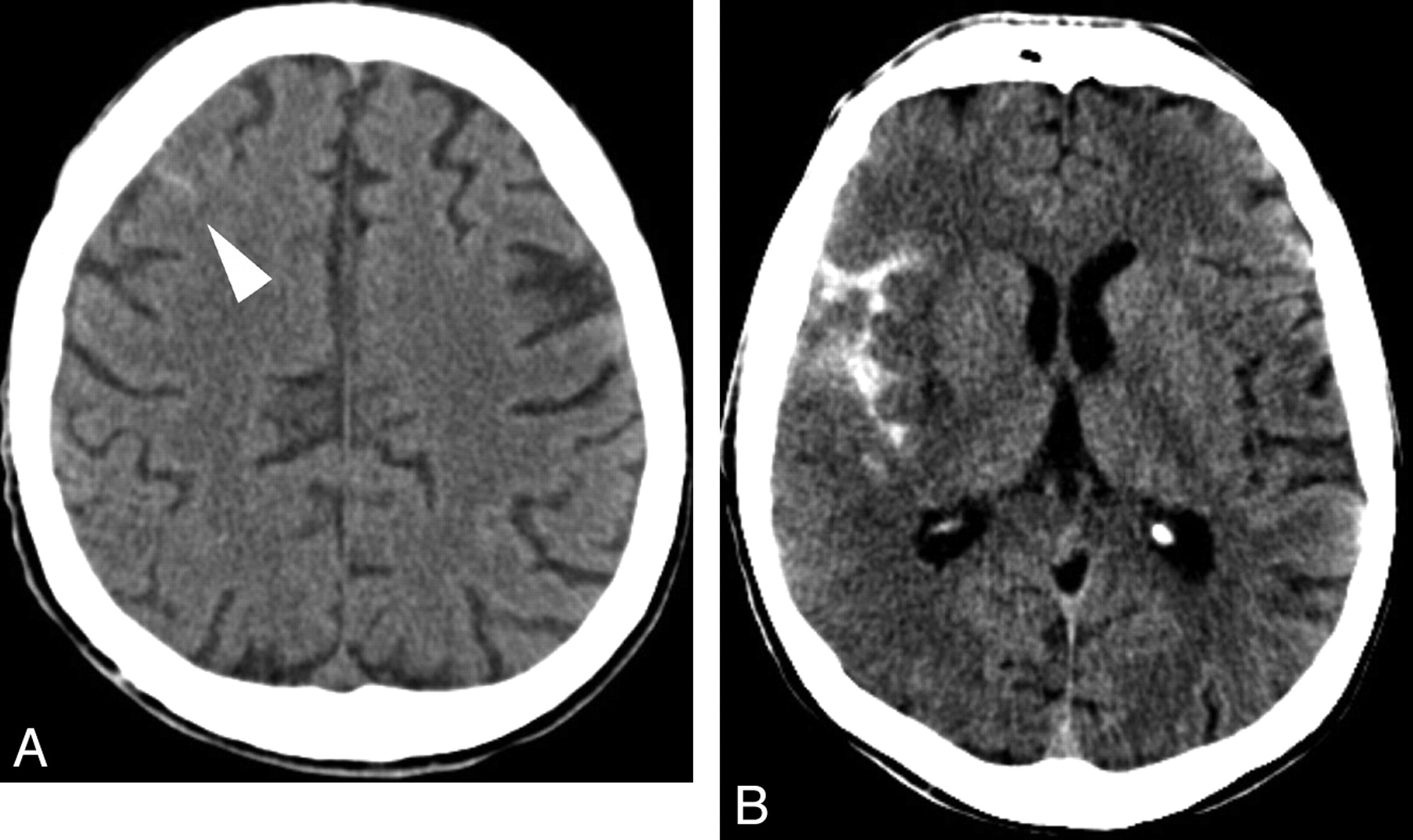
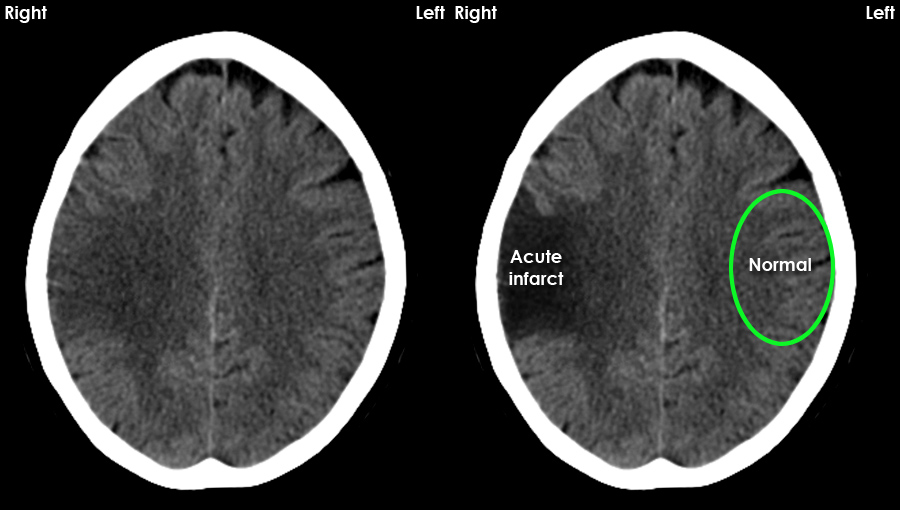
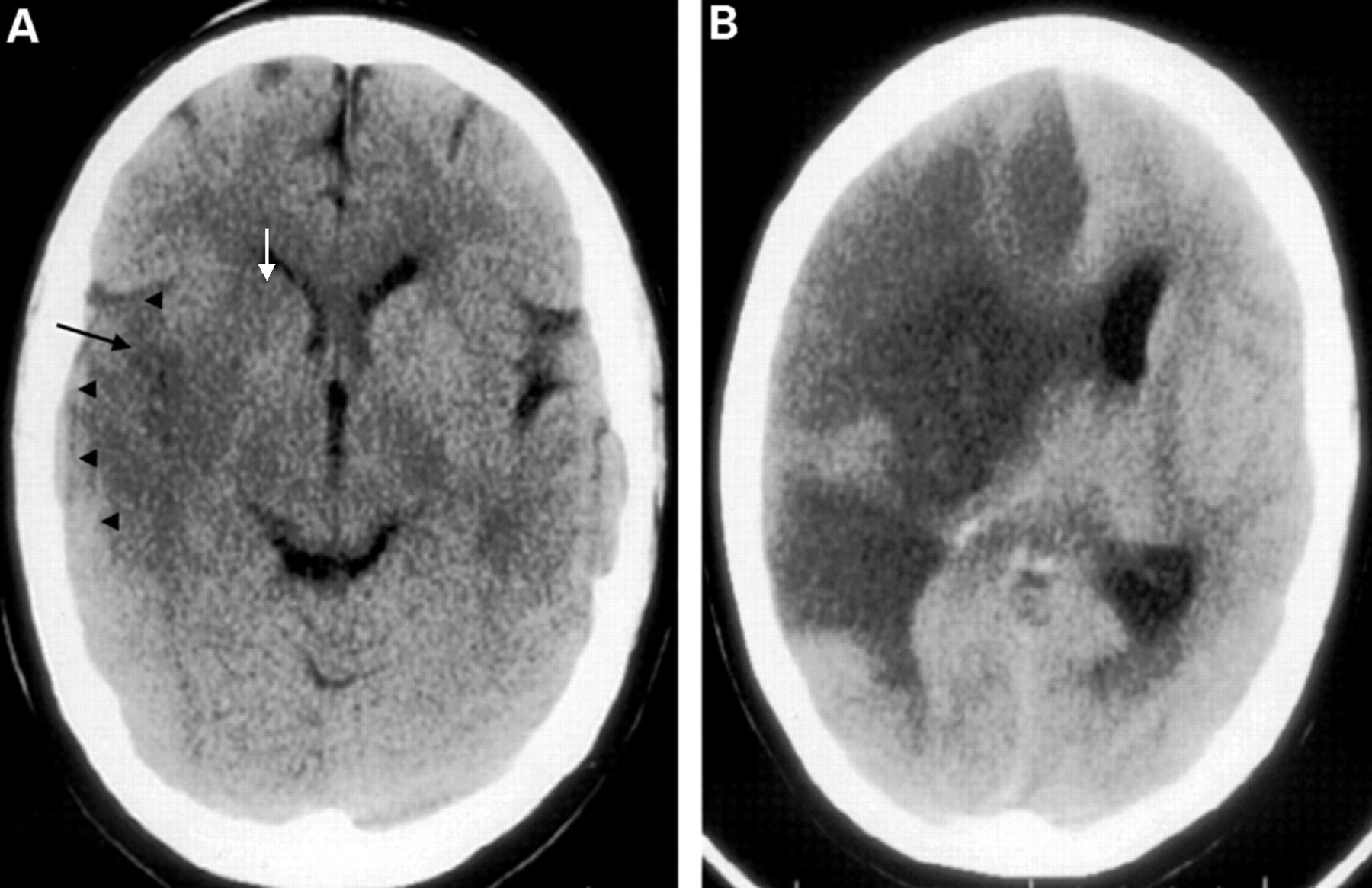
- Ischaemia: Hypodense regions in a vascular territory, loss of grey–white differentiation, sulcal effacement and early swelling.
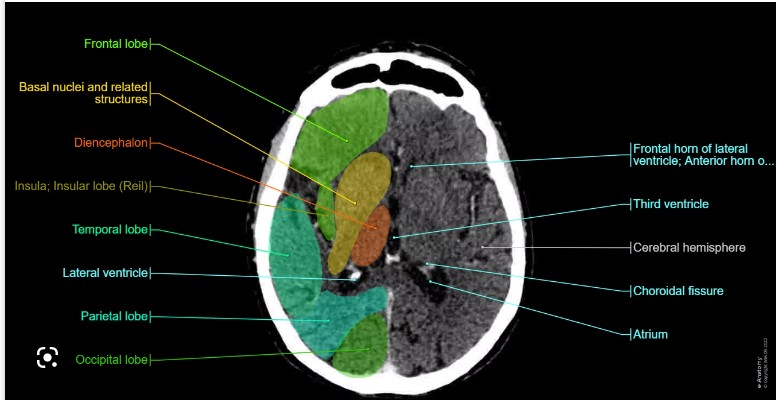
- Ventricular size: Look for dilatation, compression or asymmetry suggesting hydrocephalus, raised ICP or mass effect.
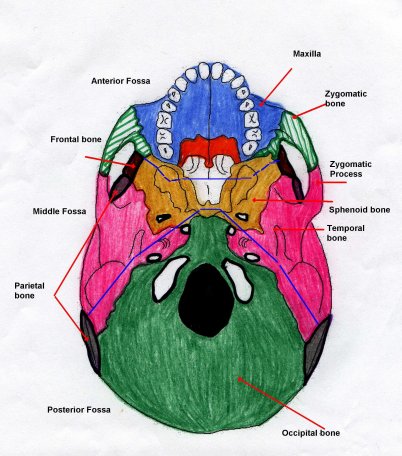
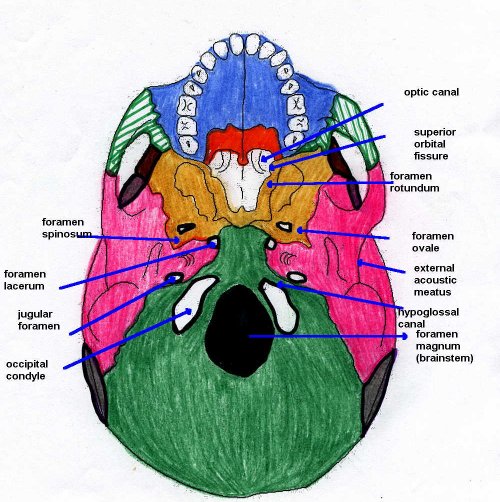
- Skull and base of skull: Fracture lines, air in cranial cavity, fluid levels in sinuses.
CT C-Spine Analysis – Key Features
For the cervical spine CT, adopt a “bones, alignment, joints, soft tissue” approach:
- Bony injury: Vertebral body, pedicle, lamina, spinous/transverse process fractures.
- Alignment: Step-offs, listhesis, abnormal angulation, loss of normal lordosis.
- Dislocations/subluxations: Facet dislocation, perched or locked facets.
- Spinal canal and cord: Canal compromise, retropulsed fragments, visible cord compression (on CT myelogram or MRI as follow-up).
- Soft tissues: Prevertebral soft tissue swelling, ligamentous injury, haematoma.
CT Features of Common Intracranial Conditions
| Condition | CT Features |
|---|---|
| Subdural haemorrhage | Crescent-shaped hyperdensity along brain surface, crossing suture lines, may track over a large area. Often associated with mass effect and possible midline shift. |
| Epidural haemorrhage | Biconvex (lens-shaped) hyperdensity that typically does not cross suture lines. May cause mass effect and midline shift; commonly related to skull fracture. |
| Intracerebral / intraparenchymal haemorrhage | Hyperdense collection within brain parenchyma with variable mass effect. Appearance depends on location and size; may extend into ventricles. |
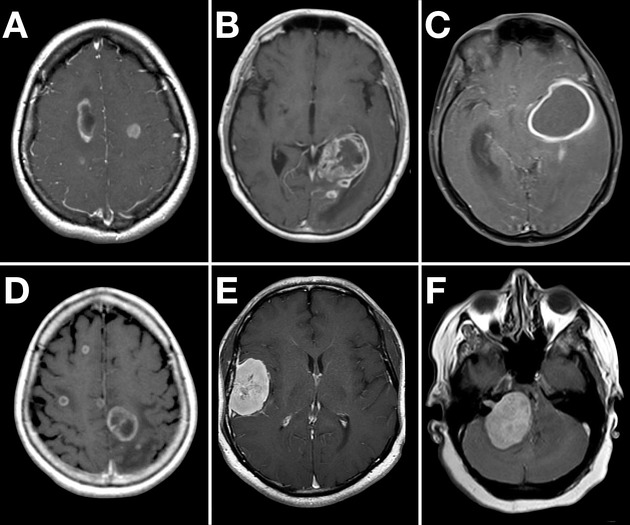
| Space-occupying lesions (tumours, metastases) | Irregular or rounded mass, often with surrounding hypodense vasogenic oedema, variable contrast enhancement, and possible midline shift. |
| Meningitis | May show sulcal effacement, diffuse or localised oedema, meningeal enhancement with contrast, and/or ventriculomegaly. CT can be normal; clinical correlation is essential. |
| Pneumocephalus | Intracranial air appearing as very low-density (black) areas, often after trauma or neurosurgery. |
| Base of skull fracture | Fracture lines through temporal bone or skull base, air–fluid levels in sinuses or mastoid air cells, possible associated extra-axial haemorrhage. |
| Subarachnoid haemorrhage (SAH) | Hyperdensity in sulci, basal cisterns, or fissures. Diffuse SAH shows widespread cortical sulcal hyperdensity; localised SAH may be focal in a specific sulcus or cistern. |
| C-spine fractures | Fracture lines of vertebral bodies or posterior elements, possible malalignment. Look carefully at occipito-cervical and cervico-thoracic junctions. |
Example CT Images (Click to Enlarge)






Intracranial Infarcts and Related Lesions – CT Features
| Intracranial Lesion | CT Features |
|---|---|
| Acute ischaemic stroke | Area of low attenuation in a vascular territory, loss of grey–white differentiation, sulcal effacement; may have mild mass effect. |
| Haemorrhagic stroke | Hyperdense intraparenchymal blood clot with or without surrounding oedema and mass effect; may have intraventricular extension. |
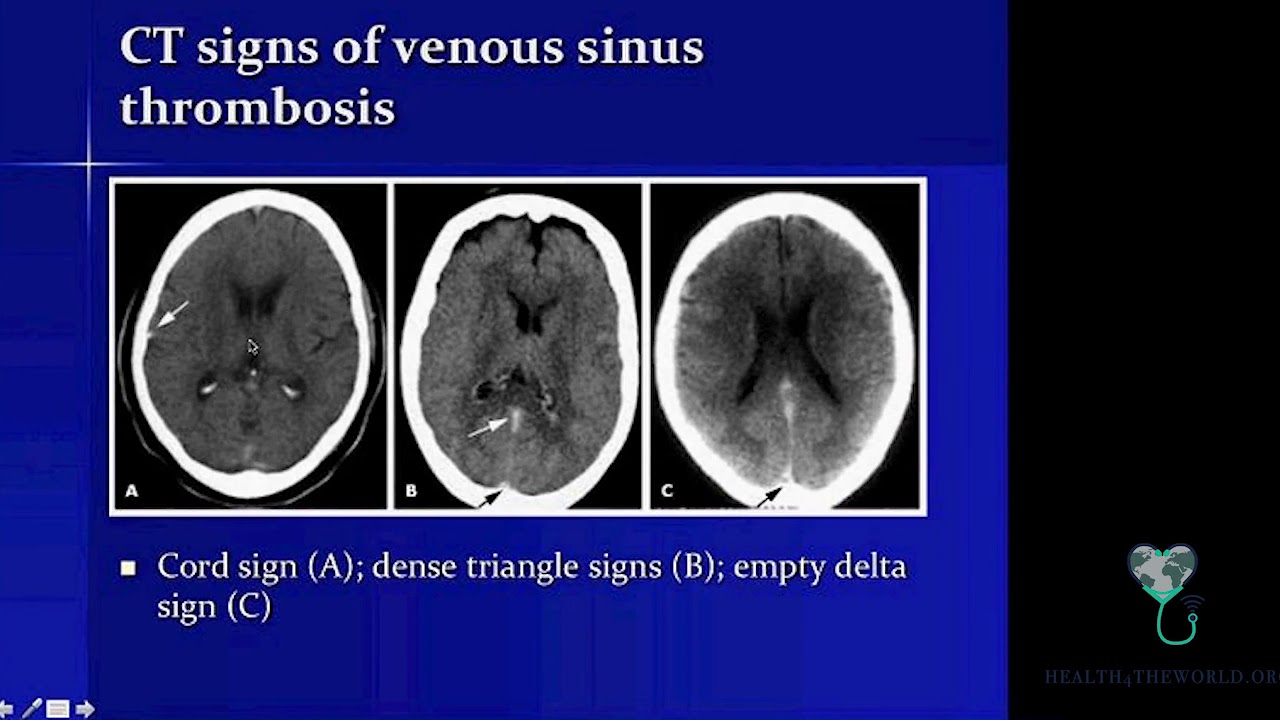
| Cerebral venous thrombosis | May show “empty delta sign” with contrast (unenhanced thrombus centrally with enhancing sinus wall), venous infarcts, or haemorrhagic venous infarcts. |
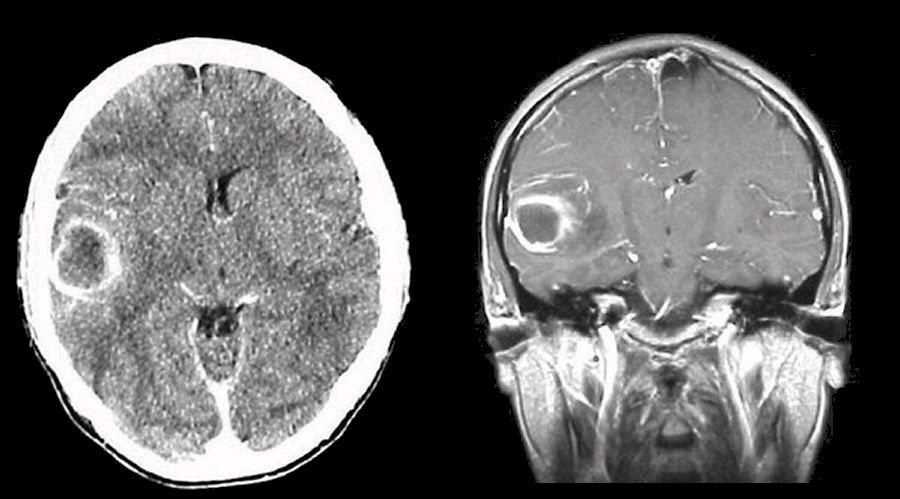
| Brain abscess | Ring-enhancing lesion with surrounding oedema; often appears as a mass lesion with central low attenuation. MRI and clinical context help distinguish from tumour. |
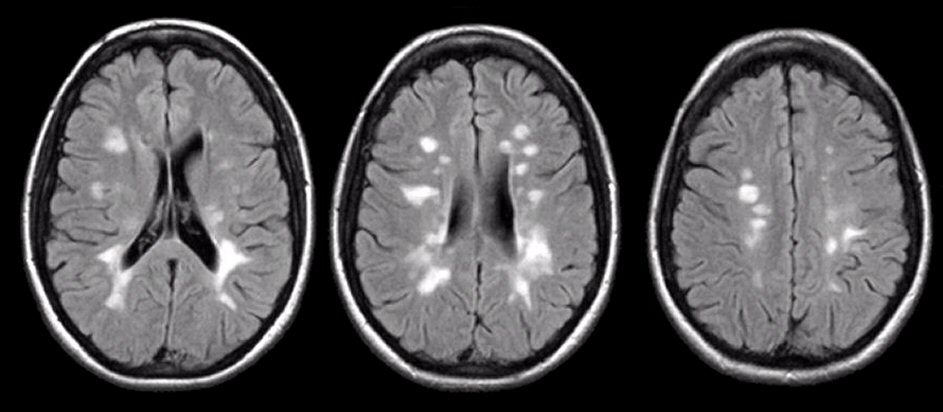
| Multiple sclerosis plaque | Well-defined low-attenuation (or subtle) lesions, often periventricular; better seen on MRI, but CT may show hypodense plaques without mass effect. |
Conclusion
CT brain and C-spine interpretation is complex and radiologist input is essential, but a structured approach allows junior doctors to identify major red flags early, prioritise management and communicate effectively with the team. Keep revisiting real cases and correlate CT findings with clinical presentation to build confidence.