Anemia Diagnosis Guide
Overview
Anemia is a condition characterised by a decrease in the number of red blood cells (RBCs) or a reduction in the haemoglobin (Hb) content of the blood. This results in reduced oxygen-carrying capacity and can lead to symptoms such as fatigue, weakness, pallor and shortness of breath.
Initial Assessment
- Obtain a detailed history: symptoms, duration, family history, diet, medications, menstrual/bleeding history, chronic illness, etc.
- Perform a physical examination: pallor, jaundice, tachycardia, murmurs, hepatosplenomegaly, lymphadenopathy, signs of chronic disease.
- Order initial laboratory tests: full blood count (FBC/CBC), reticulocyte count, peripheral smear and iron studies; consider B12/folate, renal and liver function as indicated.
Classification of Anemia
Anemia is commonly classified by mean corpuscular volume (MCV):
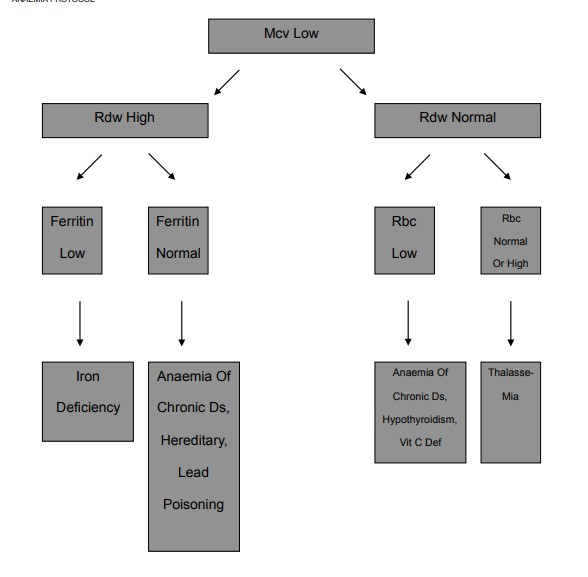
- Microcytic anaemia (MCV < 80 fL)
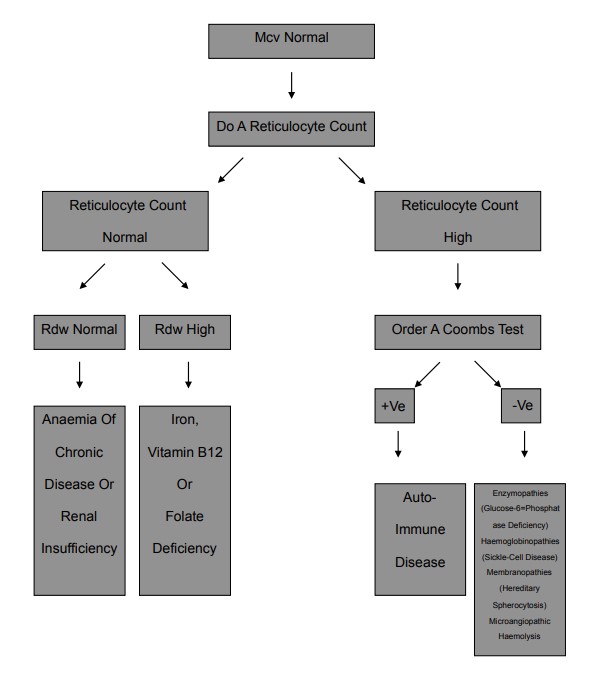
- Normocytic anaemia (MCV 80–100 fL)
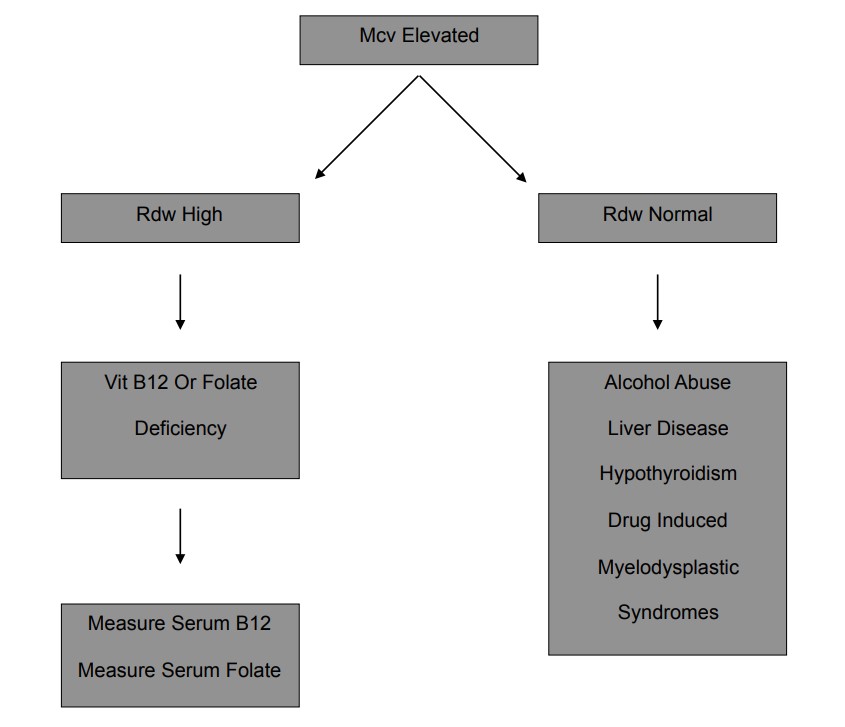
- Macrocytic anaemia (MCV > 100 fL)
Diagnosis of Different Types of Anemia
| Type of Anaemia | MCV | Key Laboratory Findings | Common Causes |
|---|---|---|---|
| Iron Deficiency Anaemia | Microcytic (MCV < 80 fL) | Low serum iron, low ferritin (or inappropriately normal if inflammation), high total iron-binding capacity (TIBC), low transferrin saturation; hypochromic microcytes on smear. | Poor diet, chronic blood loss (GI, gynaecological), malabsorption, pregnancy. |
| Thalassaemia | Microcytic (MCV < 80 fL) | Normal to high serum iron and ferritin, normal to low TIBC; target cells on smear; haemoglobin electrophoresis may show abnormal Hb patterns. | Inherited mutations affecting globin chain synthesis. |
| Anaemia of Chronic Disease / Inflammation | Normocytic (80–100 fL) or microcytic | Low serum iron, normal or high ferritin, low TIBC; often low reticulocyte count. | Chronic infections, inflammatory diseases, malignancy, chronic kidney disease. |
| Macrocytic Anaemia (usually megaloblastic) | Macrocytic (MCV > 100 fL) | Low serum B12 and/or folate in deficiency; hypersegmented neutrophils and macro-ovalocytes on smear. | Vitamin B12 or folate deficiency, malabsorption, alcoholism, liver disease, certain drugs (e.g. methotrexate, hydroxyurea). |
| Haemolytic Anaemia | Typically normocytic (may be macrocytic from reticulocytosis) | Reticulocytosis, raised indirect bilirubin, raised LDH, low haptoglobin; spherocytes, schistocytes or other abnormal cells on smear depending on cause. | Intrinsic RBC defects (e.g. hereditary spherocytosis, G6PD deficiency, sickle cell disease), autoimmune haemolysis, microangiopathic haemolysis, infections, drugs, mechanical valves. |
| Aplastic Anaemia | Normocytic (MCV 80–100 fL) | Pancytopenia, low reticulocyte count, hypocellular bone marrow on biopsy. | Idiopathic, drug toxicity, radiation, viral infections, autoimmune disease, inherited bone marrow failure syndromes. |
Treatment
Treatment of anaemia depends on the underlying cause. Address the root cause and provide supportive care:
- Iron, vitamin B12 or folate supplementation where deficient.
- Transfusions for symptomatic or severe anaemia according to local thresholds.
- Management of chronic disease (e.g. infection control, renal replacement, immunosuppression).
- Specific therapy for haemolytic anaemia (e.g. steroids, immunosuppressants, treatment of infection, stopping culprits).
- Specialist management for aplastic anaemia, haemoglobinopathies and bone marrow failure syndromes.
Anaemia Algorithms